DBSI in Prostate MRI: The Virtual Biopsy
- Describe what DBSI is trying to measure and how it differs from conventional ADC.
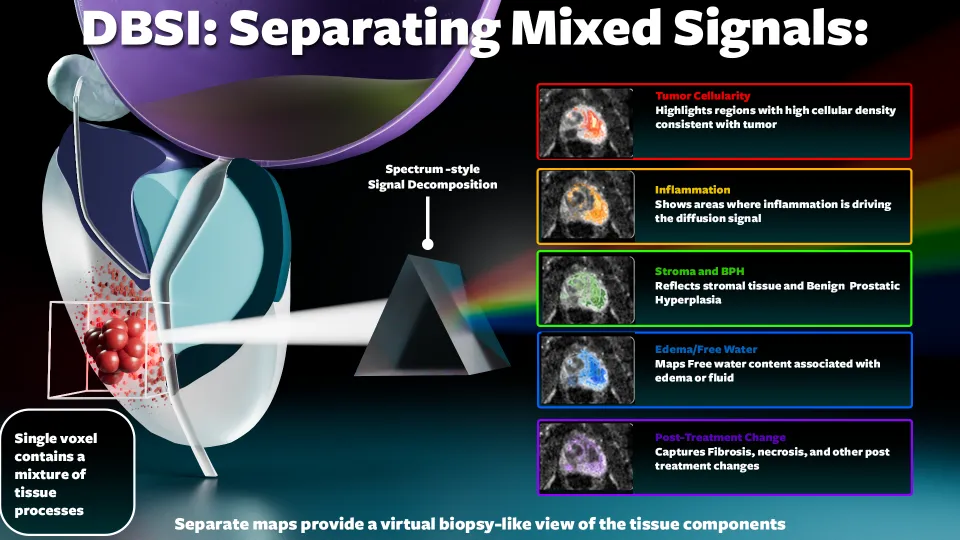
- List the four diffusion components DBSI models and the tissue environment each may reflect.
- Recognize that prostate cancer is not the only cause of restricted diffusion on ADC maps.
- Identify where DBSI fits relative to standard PI-RADS v2.1 workflow and why it is not currently part of routine reporting.
- Summarize the key finding from the 2025 study and explain why DBSI remains investigational.
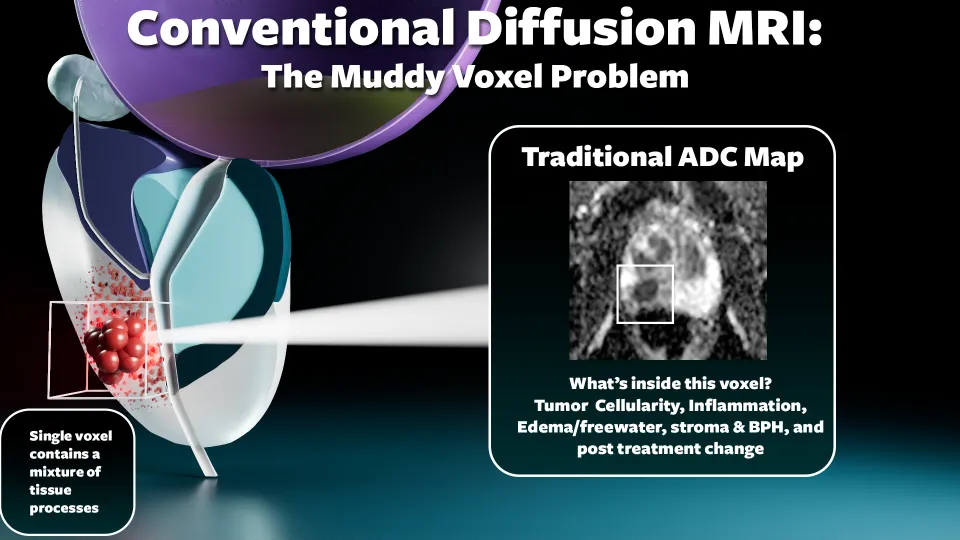
Standard prostate MRI already uses diffusion-weighted imaging and ADC maps. These images are powerful because prostate cancer often restricts water motion. But ADC is a simplified measurement; it compresses complex tissue biology into a single number. DBSI, or diffusion basis spectrum imaging, tries to go one step further.
What DBSI is trying to measure
Instead of asking, "Is water motion restricted in this region?" DBSI asks, "What mixture of tissue components may be causing the diffusion signal?"
That distinction matters because prostate cancer is not the only thing that can look dark on ADC. Inflammation, stromal BPH, fibrosis, and crowded benign glands can also alter diffusion. DBSI is being studied as a way to separate some of these overlapping signals and potentially improve risk assessment beyond conventional prostate MRI alone.
The soup analogy
DBSI is more like trying to identify the ingredients in the spoonful: noodles, meat, cream, vegetables, and broth.
In prostate MRI terms, DBSI is trying to estimate how much of the voxel behaves like restricted cellular tissue, hindered stromal tissue, or freely diffusing luminal fluid tissue.
How DBSI models a mixed voxel
DBSI models the diffusion signal within a voxel as a mixture of components. In simplified terms, these correspond to different tissue environments:
| DBSI component | Water behavior | May correspond to |
|---|---|---|
| Highly restricted diffusion | Water barely moves | Dense inflammatory cellularity |
| Restricted diffusion | Water movement is limited | Tumor cellularity or epithelial crowding |
| Hindered diffusion | Water moves but with obstacles | Fibromuscular stroma |
| Free diffusion | Water moves relatively freely | Glandular lumen or fluid |
These components are modeled mathematically from the diffusion signal, not measured directly. The tissue correspondences are biologically plausible but are still being validated.
How DBSI is acquired
DBSI is still diffusion MRI. The scanner acquires additional DBSI-specific diffusion data beyond the routine prostate DWI/ADC sequence. In other words, this is the same general family of MRI data we already use for prostate imaging, but sampled in a more specialized way.
After acquisition, DBSI post-processing uses the diffusion signal to estimate component fractions within each voxel. An AI model can then use those DBSI-derived metrics as inputs to help predict clinically significant prostate cancer.
A visual comparison: ADC vs DBSI
The diagram below shows conceptually how conventional ADC and DBSI approach a mixed prostate voxel.
tumor + inflammation + stroma + lumen
tumor + inflammation + stroma + lumen
Conceptual diagram. Component assignments are simplified and reflect ongoing research, not established clinical criteria.
How DBSI fits into the prostate MRI workflow
Current PI-RADS v2.1 interpretation is visual and pattern-based. Radiologists evaluate T2-weighted imaging, DWI and ADC, and dynamic contrast enhancement, then assign a PI-RADS category. DWI is the dominant sequence in the peripheral zone, while T2 morphology is dominant in the transition zone, with DWI able to upgrade selected lesions.
DBSI is not part of PI-RADS v2.1. It requires a separate DBSI-specific acquisition and post-processing, and its metrics are not yet incorporated into standard prostate MRI reporting systems.
Where DBSI fits next to T2 and ADC
| Feature | T2-weighted MRI | DWI / ADC | DBSI |
|---|---|---|---|
| What it evaluates | Tissue morphology and signal intensity | Average water diffusivity within the voxel | Estimated mixture of diffusion components within the voxel |
| Output format | Visual signal pattern | Single ADC value (mm²/s) | Component fractions: restricted, hindered, free |
| Part of PI-RADS v2.1? | Yes (dominant in TZ) | Yes (dominant in PZ) | No. DBSI requires DBSI-specific diffusion acquisition and post-processing, and is not part of PI-RADS v2.1. |
| Available for routine use? | Yes | Yes | Research implementation. Can be performed on clinical scanners when the DBSI protocol and post-processing pipeline are available, but it is not routine prostate MRI. |
| Validated for routine clinical use? | Yes | Yes | Still investigational |
| Main limitation | Overlap between BPH, inflammation, and cancer on signal alone | Compresses complex tissue biology into one number; does not separate overlapping causes of restriction | Requires dedicated acquisition and post-processing; results not yet standardized or broadly validated |
Why this could matter for PI-RADS 3 lesions
A PI-RADS 3 lesion is indeterminate. Some are clinically significant cancers, but many are not. One of the persistent challenges in prostate MRI is knowing what to do with equivocal findings: biopsy all of them, follow some, or use additional information to refine the decision.
DBSI may eventually help risk-stratify equivocal lesions by estimating whether the diffusion abnormality is more tumor-like, inflammatory, stromal, or fluid-rich. If the signal in a PI-RADS 3 lesion looks primarily like hindered stromal or free luminal components, that might eventually support a lower biopsy urgency. If it looks more like restricted cellular signal, that might increase concern. This remains investigational.
What the recent 2025 study showed
A 2025 Journal of Urology study evaluated DBSI in 241 patients who underwent prostate MRI with both conventional and DBSI-specific sequences before biopsy. The authors applied artificial intelligence models to DBSI metrics and used biopsy pathology as the reference standard.
In that study:
- The DBSI-based AI model was an independent predictor of clinically significant prostate cancer.
- DBSI alone performed similarly to the combination of PSA density and PI-RADS in that dataset.
- The combination of DBSI and PI-RADS had the highest reported discrimination, with an AUC of 0.894.
- In a modeled strategy using DBSI for patients with PI-RADS 1 to 3 findings, biopsies could have been reduced by 27%, while missing 2% of clinically significant cancers compared with biopsying all patients.
What DBSI cannot do
DBSI should not be interpreted as a replacement for standard prostate MRI interpretation. It does not eliminate the need for:
- High-quality T2-weighted imaging, DWI, ADC, and DCE when appropriate
- PI-RADS v2.1 assessment
- PSA density, biopsy history, and clinical judgment
- Shared decision-making between urology and radiology
DBSI should not be described as a proven way to avoid biopsy in routine clinical practice. It is an area of active investigation. Implementing it clinically would require appropriate DBSI sequences, validated AI models, and institutional or multi-site validation data that do not yet exist on a broad scale.
Teaching takeaway
DBSI tries to explain what type of tissue mixture may be causing that restriction.
Bottom line
DBSI is an emerging diffusion MRI technique that attempts to extract a more detailed microstructural fingerprint from prostate tissue than conventional ADC alone. Early work suggests that DBSI-derived metrics, especially when combined with AI and PI-RADS, may improve prediction of clinically significant prostate cancer and could potentially reduce unnecessary biopsies.
For now, DBSI should be viewed as promising but investigational, not yet ready for routine clinical implementation or PI-RADS reporting.
Related tools and articles
References
- American College of Radiology, European Society of Urogenital Radiology, and AdMeTech Foundation. PI-RADS® v2.1: Prostate Imaging - Reporting and Data System. Version 2.1. 2019.
- Oerther B, et al. Cancer detection rates of the PI-RADSv2.1 assessment categories: systematic review and meta-analysis. Prostate Cancer and Prostatic Diseases. 2022.
- Kim et al. Artificial Intelligence Model Using Diffusion Basis Spectrum Imaging Prostate MRI to Predict Clinically Significant Prostate Cancer. Journal of Urology. 2025.
- National Cancer Institute. Clinical trial: DBSI prostate cancer imaging (NCI-2020-04492).
- ISMRM 2018 Proceedings. WashU/ISMRM DBSI / prostate D-Histo abstract. Abstract 0722.